Pressing pause on low-grade gliomas: The long road to a breakthrough treatment

When asked about his many failed attempts to invent a new type of storage battery, Thomas Edison famously quipped, “I have not failed. I’ve just found 10,000 ways that won’t work.”
It’s a feeling cancer researchers know well, particularly those dedicated to eradicating brain tumors, who have faced decades of disheartening defeats and persistent roadblocks.
Elizabeth Maher, M.D., Ph.D.
“Our path is littered with failed clinical trials and it’s not for lack of trying,” notes physician-scientist Elizabeth Maher, M.D., Ph.D., a Professor of Internal Medicine and Neurology at UT Southwestern, member of the Peter O’Donnell Jr. Brain Institute, and holder of the Theodore H. Strauss Professorship in Neuro-Oncology. “We have amazing clinical trials teams, but for a time, everything we picked was an abject failure. So you have to be somewhere where you can do the investigation and really push the underbelly of the whole thing to figure out what’s the problem.”
For more than 20 years, Dr. Maher and her colleagues have endured many setbacks in their pursuit of effective treatments for brain tumors. With each disappointment, however, her team continued chipping away at barriers, rethinking priorities, and developing new testing methods. While progress wasn’t always constant, the researchers gathered further resources and learned much more about the nature of different brain tumors, leading to innovations in resources and experiment methods.
Until finally, everything they had worked on began to fall into place.
Timing is everything
In 2024, the Food and Drug Administration (FDA) approved an oral drug called vorasidenib (brand name Voranigo) to treat low-grade gliomas, a type of brain tumor formed from glial cells. This drug was found to lock these tumors in a dormant state for longer, preventing them from turning into deadly high-grade gliomas and potentially adding years to a patient’s lifespan. With the benefit of significant extra time, researchers can continue working toward their ultimate goal of eradicating brain tumors entirely.
It’s a landmark achievement for countless patients, made possible thanks to efforts across UT Southwestern and the broader medical community, which gave clinicians and researchers all the elements they needed to make a groundbreaking discovery at just the right time.
Mapping the path to that discovery highlights a journey of sporadic innovation that forced cancer researchers to refine their approaches to testing, specimen collection, and even which types of cells to target with their research, ensuring the right pieces were aligned for a breakthrough.
The right place: Creating a supply chain for tissue samples
One of the largest challenges when researching brain tumors in general is obtaining live tissue specimens. Depending on the location of the tumor, performing a biopsy can be too risky, which typically leaves only two opportunities to access cancer cells from a patient: during the initial surgery to remove the tumor and during a second surgery, if the cancer recurs. For some tumor types, such as dormant glioblastomas, researchers can’t collect samples once the patient has started chemo and other treatments. Because of these restrictions, building and maintaining a comprehensive bank of cancer cells is essential for ongoing testing.
With UT Southwestern’s research labs and medical treatment centers essentially next door to each other, Dr. Maher and her colleagues could easily collaborate in real time with their clinical partners – particularly the neurosurgeons, neuropathologists, and others who were equally committed to advancing tumor research – to gather specimens. This open-door, team-based approach gave them frequent opportunities to collect samples from patients already undergoing surgical procedures to remove the same types of tumors they were studying.
“Working specifically with tissue from the operating room, getting a tumor from the exact patient whose tumor type we are studying, that’s a gigantic critical resource available here, and it requires that the patients partner with you to allow you to do that,” Dr. Maher says. “I always tell patients, ‘Maybe there’s already a drug out there that works, but we wouldn’t know because we’ve never had the opportunity to study those cells in hand.’”
Accessing specimens directly from patients enables researchers to gather a variety of cancer cells for different types of tumors, states of activity, mutations, and other variables. However, this method still only provides them with a finite amount of cells to work with – once they’re used up for testing, they’re gone. To achieve a real breakthrough, researchers must ensure a steady supply of samples for any type of cancer they decide to focus on.
Robert Bachoo, M.D., Ph.D.
Fortunately a $3.2 million donation from the Moncrief family provided neuro-oncologists at UT Southwestern with the exact resource they needed. With those funds, Robert Bachoo, M.D., Ph.D., Associate Professor of Neurology and Internal Medicine at UT Southwestern and Dr. Maher’s husband, established a robust mouse model to propagate more samples. By inserting tumor cells into mice, neuro-oncologists can now cultivate whole colonies of any cancer type obtained from a patient.
With an ample supply of tissue samples in hand, researchers had the means to hone their efforts on even more specific types of cancer and pursue some less conventional directions that typically don’t get as much attention in research labs.
The right cells: Exploring dormancy and migration
For decades, cancer research and drug discoveries have mainly targeted active tumor cells that are consistently dividing and spreading, since those tend to pose the most imminent threat to a patient’s life. However, even if the active cells are successfully eliminated through chemotherapy, radiation, or surgery, there’s still a possibility of dormant cells remaining or even migrating to other parts of the body to begin multiplying again. Oftentimes, a recurring tumor from these cells is what ultimately ends a patient’s life.
In the case of certain brain tumors, such as low-grade gliomas and post-treatment glioblastomas, the cancer cells can remain dormant for two to five years, causing few issues. During this time, doctors must monitor patients’ scans for any changes but cannot provide much treatment. Once the cancer cells begin actively replicating, the same tumors can quickly become aggressive and form into a much more dangerous high-grade glioma or recurrent glioblastoma. Whatever causes this switch is still unknown, and unveiling the mechanisms behind it is a complex challenge.
“Let’s say you could go to the operating room and get those very low-grade cells and bring them back to the lab. You put them in a dish; they don’t grow – they die,” Dr. Maher explains. “You could take them and put them directly into the brain of a mouse, like we do with high-grade cells. They don’t grow; they don’t make a tumor. The problem is, you can’t study something that doesn’t grow.”
For researchers, investigating dormancy in cancer cells could be the key to stopping their progression, and low-grade gliomas present an excellent model to study. Targeting low-grade tumors is not only valuable for understanding these specific tumors but also teaches neuro-oncologists about the dormant state in other cancers, such as post-treatment glioblastomas.
What’s more, these dormant cells can migrate within the brain, moving between cells and along nerve fibers, potentially causing a recurrence elsewhere and posing a worse risk than before.
According to Dr. Maher, “You don’t want these cells to move, because patients go in and have an initial surgery that might be in an area of the brain that’s safe. Then they’re doing well and living their life, but next thing, it reappears on the other side of the brain or in an area that controls a critical brain function like walking or speaking.”
The right platform: Developing microwells and microchannels
Microchannels: for spontaneous 3D single cell migration. Seeding chamber bottom right and exit chamber top left.
While the researchers had identified dormant and migrating cells as a potential target for cancer treatments, they still had no effective means to study them in a lab setting. They would have to develop new methods to observe and test them – not an easy feat considering these cells, by definition, show little to no activity.
Once again, Dr. Bachoo stepped in, this time partnering with bioengineers at UT Arlington. Drawing on UT Southwestern’s support for faculty innovation, they invented and patented microwell and microchannel platforms to simulate the brain environment these single cells usually live in, with slight variations to induce different behaviors.
For a dormancy assay, samples could be placed in a 1-by-1-centimeter macrowell consisting of 80,000 microwells. With each microwell measuring almost exactly the size of one cell – 15-by-15 micrometers (µm) – an individual cell has no room to divide, effectively forcing them to remain dormant, but alive for observation. Dr. Bachoo also created a clonogenic assay version, with one macrowell holding 11,500 microwells measuring 50-by-50 µm each, giving single cells space to grow a little so scientists could observe their behavior when dividing.
“Studying cancer at a single cell level gives you more information,” Dr. Maher says. “Even though they’ll still just sit there, they’ll behave the same way as a low-grade cell. You can then do genetic sequencing, proteomics, and all the things scientists focus on. You can do all of that and discover what pathways might be the Achilles’ heel of the cell to target.”
Likewise, Dr. Bachoo created a dynamic migration assay with microchannels measuring the width of one cell but with a much longer length. Placing cells in these microchannels allows researchers to label them with fluorescent dye and observe how they behave when given room to move. Under these conditions, researchers have been able to mimic the paths tumor cells use to travel locations and influence them to migrate.
The introduction of microchannels and microwells into research labs opened the door for more effective single cell testing during the dormant and migrating phases. Doctors gained much greater insight into how tumors, from low-grade gliomas to high-grade glioblastomas, proliferate in the brain, even after treatments.
“We were just dying to know the answers to some critical questions,” Dr. Maher says. “‘Is the reason these cells come back because they were hiding in the channels of the brain? Does chemo and radiation kill the cells in the channel? And does it kill them when they’re dormant sitting there?’ And the answer is no, they don’t care at all. You apply treatment, and they still ride along nice as you like. It’s a huge piece of knowledge that was missing. So, if we can’t get the right drug for the initial or the recurrent tumors, maybe we go after these dormant cells and kill them that way.”
Now that the team had a greater understanding of low-grade cancer cells and how to test with them, the next step was to connect that knowledge to a viable treatment for patients. More importantly, they needed a narrower bull’s-eye – a more specific cancer type they could confront directly. Fortunately, Dr. Maher had already worked extensively with the exact form of cancer they needed.
The right target: Tracking the IDH mutation with advanced imaging
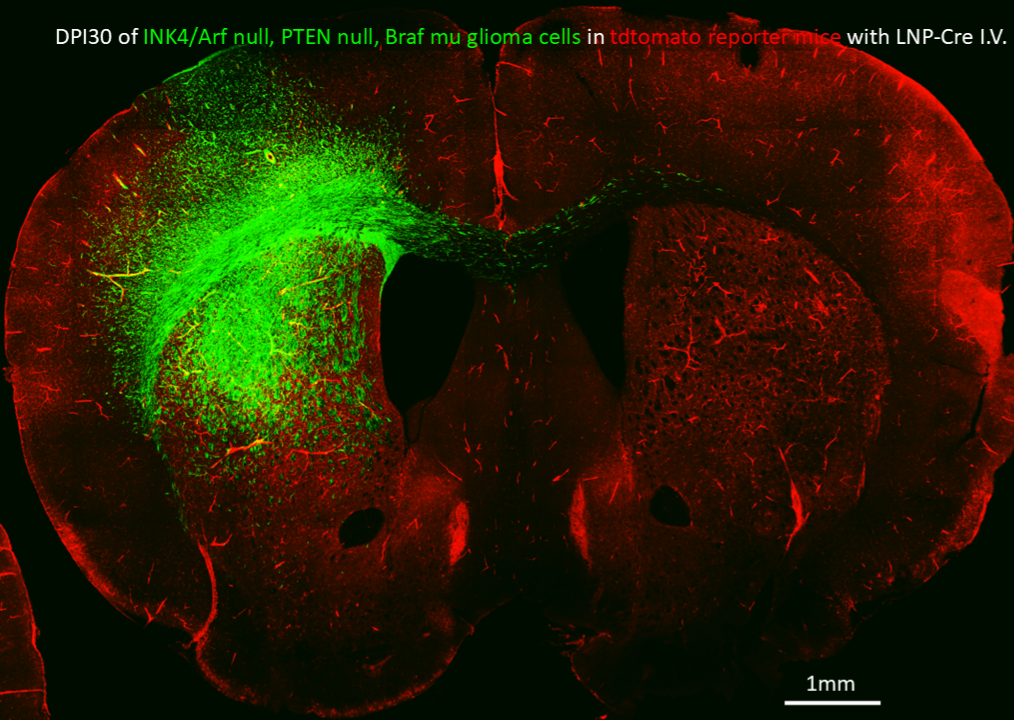
Green cells migrating in the brain of a mouse.
In 2008, scientists identified a mutation in some cancer cells affecting isocitrate dehydrogenase (IDH), an enzyme that typically metabolizes glucose. In mutated cells, IDH could disrupt cellular activity, influencing whether cancerous cells grow or migrate. Researchers later determined the disruptions were partly caused by 2-hydroxyglutarate (2HG), a molecular byproduct that accumulates in these cells. If they could accurately and safely detect 2HG levels in patients, researchers reasoned, they could not only identify an IDH-mutated cancer without surgery but also track its progress more predictably to provide more effective interventional treatment.
Almost a decade after the IDH mutation’s discovery, Dr. Maher put this theory to the test and collaborated with Changho Choi, Ph.D., a former Associate Professor in UT Southwestern’s Advanced Imaging Research Center (AIRC). Dr. Choi was experimenting with a new 7 tesla (7T) MRI machine, providing more than twice the imaging clarity of a typical 3T machine. With advanced imaging capabilities, the two hoped to find a noninvasive biomarker to indicate when dormant cancer cells were about to become active. During their research, Dr. Choi developed a protocol to measure the chemical signature of 2HG, enabling doctors to track a patient’s levels more closely along with their cancer’s progression. As an IDH-mutated tumor grew, so too did the body’s 2HG levels; but if the patient started chemo or other treatments, their 2HG would drop. Further research found this was true for both IDH-mutant glioblastomas and low-grade gliomas.
Finally, doctors could track this specific type of brain tumor’s growth without surgery. Now they would just need to apply that knowledge to develop more impactful treatments. When discussing the IDH mutation back in 2018, Dr. Maher was quoted as saying, “This is a solvable problem. You just need the right mix of people and a little bit of good luck.”
She did not know it yet, but that “good luck” was just a few years away.
The right time: Piecing it all together
After accumulating the resources to test and track IDH-mutated cell growth, Dr. Maher led UT Southwestern’s participation in multicenter trials for a first-of-its-kind IDH inhibitor called ivosidenib. Like many drug trials aimed at brain tumors in the past, the pharmaceutical company and researchers hoped to prove the drug as an effective treatment for high-grade glioblastomas.
They theorized that suppressing the IDH mutation would prevent the cancer cells from replicating but were not sure how the drug would fare against tumors in actual patients. For the trials, Dr. Maher’s team enlisted a group of eligible IDH-mutant glioblastoma patients but permitted several IDH-mutant low-grade glioma patients to enroll as well.
Although the drug had shown results in lab tests, the company’s chemists were skeptical that it would even be able to cross the blood-brain barrier at high enough levels to affect the tumors. This wouldn’t be an issue for glioblastoma patients, as their blood-brain barriers are typically weakened, allowing medication to cross freely. Low-grade glioma patients, on the other hand, usually have an intact blood-brain barrier, which could render the drug useless for regular treatments.
Initially, the trials appeared to be a failure. Months after patients started the drug, ongoing scans showed the IDH-mutant glioblastomas, the primary target of the trials, continued to grow unabated. It turned out that past a certain point, the IDH mutation was no longer a factor in the tumor’s expansion, meaning ivosidenib had no effect on these patients. As Edison might say, they had discovered one more way that would not work.
The pharmaceutical company came close to scrapping the trials entirely, until Dr. Maher’s team stepped in with some unexpected results. Using the advanced imaging techniques created by Dr. Choi, the UTSW researchers discovered reduced 2HG levels in the IDH-mutant glioblastoma patients. The drug had crossed their weakened blood-brain barriers as expected; it just didn’t prevent the tumors from growing. But they weren’t the only patient cohort affected.
For the small number of low-grade glioma patients, although their tumors didn’t show much activity – as is typical – they showed reduced 2HG levels as well. For them, the drug had successfully crossed the intact blood-brain barrier and hit its target.
In one moment, everything cancer researchers had learned about IDH-mutant cancer cells in the brain culminated in Dr. Maher’s lab. UT Southwestern now had the only proof that the drug worked, just not in the patients they expected. Low 2HG levels proved that the drug had crossed the blood-brain barrier and hit its target in the low-grade glioma patients. For the first time ever, there was a drug in hand that could be used on slow-growing tumors. Dr. Maher’s team even showed that the tumors stopped growing for months while patients were on the drug – but they still needed more clinical trials to prove it.
As Dr. Maher explains, “Because of our imaging, we were able to say, ‘Wait a minute. You’re ready to throw this drug out because it’s not working? We’re targeting the wrong patient population in the trial.’”
The company and other investigators agreed to keep going, but this time focusing on the low-grade glioma patients.
With the backing of UT Southwestern’s Institutional Review Board (IRB), the team continued clinical trials, this time using an improved version of the drug called vorasidenib, which crossed the blood-brain barrier at 10 times the concentration of ivosidenib. Through placebo testing and imaging, they were able to confirm their suspicions: The drug couldn’t outright kill cancerous cells, but it would stop their growth. So long as a patient started medication during an IDH-mutated tumor’s dormant phase, before it progressed to high grade, the drug could add years to their survival.
Further testing showed the drug suppresses the cancer cells’ ability to migrate. The low-grade tumors remain, but as long as the patient continues taking the drug, they will not grow or have the chance to move anywhere else in the brain.
In 2023, the team received its biggest win yet. In the middle of testing, the FDA determined the benefits of vorasidenib to patients were too great to ignore and ended the trial early. On Aug. 6 that year, the FDA officially announced vorasidenib could be prescribed to treat low-grade gliomas in adults and children ages 12 and older following surgery.
For patients typically told they may only have a few years left to live, this was the best news in decades. It was the culmination of dedicated effort on the part of countless physicians and patients and a testament to how the right resources at the right time can make all the difference.
‘Frontier mentality’ at UT Southwestern
Dr. Maher credits this most recent breakthrough treatment to UT Southwestern putting mechanisms in place to push cancer research forward and giving researchers the freedom to “follow the science” down any avenue they could.
“When [Dr. Bachoo] and I were being recruited in 2005, I remember Greg Fitz, M.D., who was the Chair of Internal Medicine at the time, said to me, ‘You know, UT Southwestern still has that frontier mentality. Come here, do your work. We’ll all help you.’ And that’s always been true. You always have a seat at any table you want to be at.”
Fortunately, the methods and developments that led to vorasidenib’s FDA approval can readily apply to other cancer types, particularly glioblastomas. Surgeons and pathologists across UT Southwestern continue to collaborate closely to identify and collect new cancer cell types. Thanks to the expanded mouse models, researchers have a steady supply of tissue samples for testing.
Drs. Maher and Bachoo are continuing to refine microwell and microchannel platforms to open new approaches for studying both low- and high-grade cell behavior. Building on previous findings, a team of researchers at UT Southwestern, including Drs. Maher and Choi, published a paper describing a method to diagnose IDH-mutant gliomas in the brainstem without requiring a biopsy, a typically risky procedure for that area of the body. With a recent $2 million donation from the Snyder Foundation – created in honor of Stacey Snyder, a Dallas-based boxing photojournalist who died from a glioblastoma – they are also expanding their research into migrating cells to help prevent recurrent tumors.
As far as Dr. Maher is concerned, the next frontier in brain tumor treatment is discovering a new critical pathway to target, much like the IDH mutation. Now that they’ve proved dormant and migrating cells can be effectively studied and tested in the lab, scientists can coordinate further drug trials to find the next treatment.
The main goal is to eliminate dormant and migrating cells entirely, not just hold them in place, and prevent them from recurring.
“Dormant is good. Dead is better,” Dr. Maher says. “We don’t want them to be alive to fight another day. So a large part of the focus is: You’ve got them inhibited; now how do you kill them?”